
Artificial intelligence is making headlines in healthcare — again. This time, it’s not about chatbots scheduling appointments or AI reading X-rays a bit faster. It’s about something bigger, more disruptive, and potentially far more consequential: AI outperforming doctors in making complex diagnoses.
Microsoft recently released findings showing that their AI Diagnostic Orchestrator (MAI-DxO) correctly solves up to 85.5% of cases published in the prestigious New England Journal of Medicine — outperforming experienced physicians who scored, on average, around 20%. On paper, this is nothing short of extraordinary. AI, they argue, can now mimic — and even surpass — human diagnostic reasoning in medicine’s most demanding cases.
But amid the excitement, there’s an uncomfortable question healthcare leaders must confront: Are we moving too fast in handing over clinical judgment to machines?
In this article, we’ll break down what’s happening in the AI-driven diagnostic space, explore the real implications for hospitals, insurers, and clinicians, and highlight not only the promise but also the hidden costs, risks, and ethical dilemmas that come with this rapidly evolving technology.
The Race Toward Diagnostic Superintelligence
The shift toward AI-assisted diagnosis isn’t coming — it’s already underway.
Microsoft’s research showcases the growing maturity of generative AI in handling complex clinical reasoning. Unlike earlier AI benchmarks that tested models on medical licensing exams or symptom checkers, their new benchmark — the Sequential Diagnosis Benchmark (SD Bench) — simulates real-world diagnostic journeys. It presents the AI with step-by-step clinical information from NEJM case reports, mimicking how doctors actually reason through uncertainty: asking questions, ordering tests, and updating hypotheses.
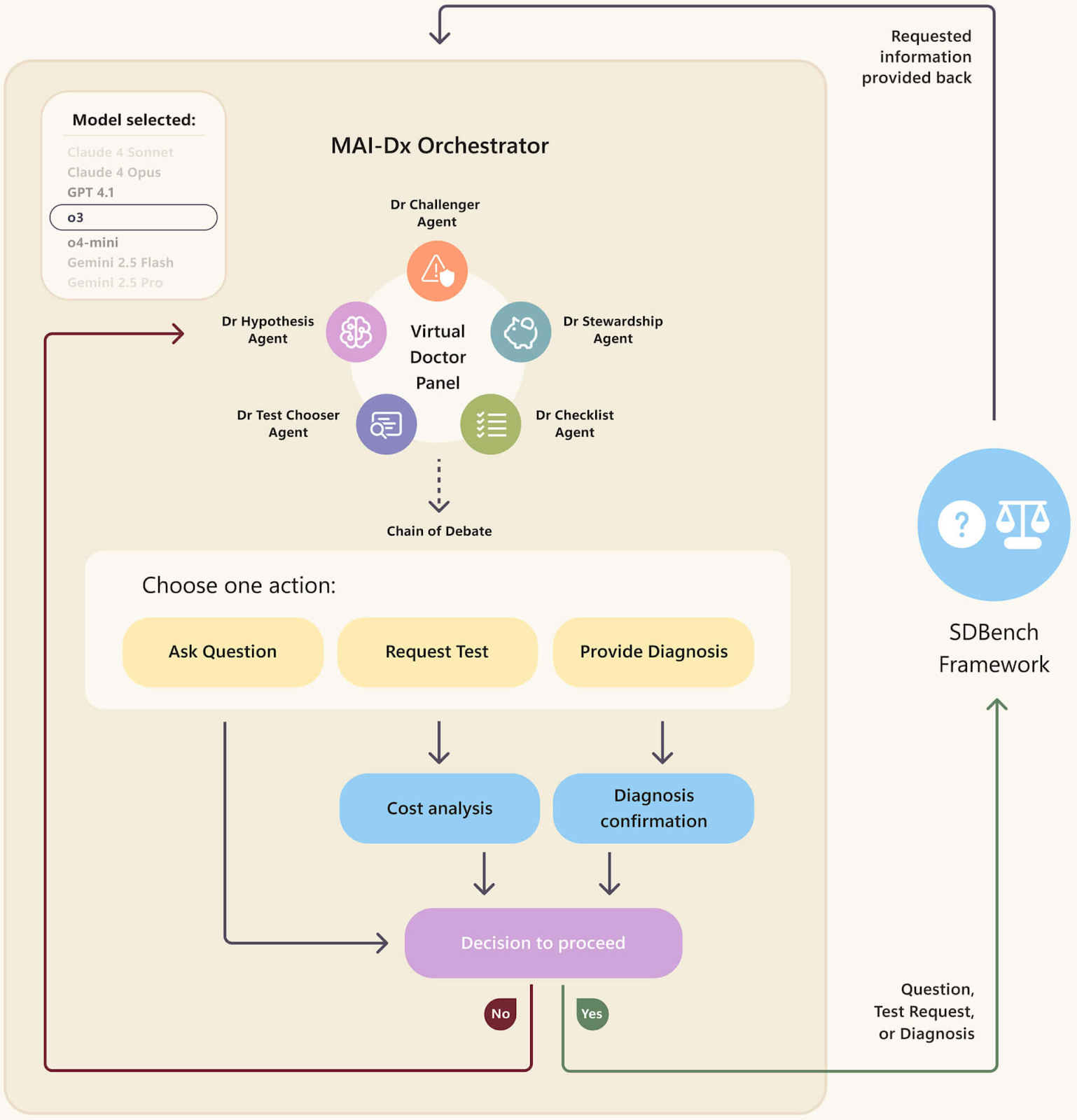
The MAI-Dx Orchestrator transforms a language model into a simulated team of doctors — capable of asking follow-up questions, recommending tests, and issuing diagnoses. It can also assess costs and double-check its own logic before taking the next step.
This is a major leap forward. Traditional benchmarks relied heavily on multiple-choice questions, which favor memorization and pattern-matching. But real medicine rarely presents itself in a tidy list of four options. Instead, it unfolds through incomplete, noisy, and sometimes contradictory information.
Microsoft’s MAI-DxO addresses this by acting like a virtual diagnostic team, orchestrating multiple AI agents that simulate different lines of medical thinking. As new clinical details become available — say, a lab result or a patient’s history — the orchestrator adjusts its working diagnosis. It can even consider the cost of each test, making it theoretically more efficient than both doctors and standalone AI models.
The result? According to Microsoft, MAI-DxO not only delivers superior accuracy but does so at a lower diagnostic cost.
It’s a compelling pitch. But it’s also a partial one.
The Other Side: What AI Can’t (Yet) Do
Beneath the surface of these performance numbers lie unanswered questions that healthcare decision-makers must not ignore. For all its impressive results, MAI-DxO — and AI systems like it — are not yet ready for uncritical deployment in clinical settings. In fact, depending on how they’re integrated, they could introduce new vulnerabilities that put patients at risk.
1. Contextual Blindness
One of the most serious limitations of current AI models is their lack of contextual understanding. AI doesn’t know what it doesn’t know. While humans reason through uncertainty by drawing on experience, emotional nuance, and environmental context, AI models reason based on patterns in their training data.
This becomes dangerous in edge cases — especially in underrepresented populations. If a diagnostic AI has been trained mostly on Western, hospital-based data, it may underperform in rural clinics, pediatric settings, or low-income environments where symptoms present differently or care pathways deviate from the norm.
2. The Illusion of Objectivity
It’s tempting to believe that AI is neutral, clinical, and devoid of bias. But that belief is itself a bias. AI is only as objective as its inputs — and the medical field is full of historical biases.
For example, research has shown that pulse oximeters — and by extension, AI systems trained on their data — are less accurate in patients with darker skin tones. Similarly, many diagnostic algorithms are built on datasets where women, minorities, and people with disabilities are underrepresented.
Without intentional bias correction and diverse training data, AI risks perpetuating and scaling the very inequities it claims to solve.
3. Overtrust and Automation Bias
Another real concern is what psychologists call automation bias: the tendency to trust a machine’s output, even when it’s wrong.
In a high-pressure clinical setting, where time is scarce and decision fatigue is common, there’s a strong temptation to defer to the AI — especially if it’s been advertised as outperforming human doctors. But overtrusting AI can be just as dangerous as ignoring it. If a machine misses a subtle red flag — or worse, confidently offers a wrong diagnosis — and no one challenges it, the result can be catastrophic.
4. Lack of Explainability
Most generative AI systems, including Microsoft’s MAI-DxO, operate as “black boxes.” They can output a diagnosis, even walk through a reasoning process, but they don’t truly “understand” anything. Their reasoning is a statistical echo of the data they were trained on — not the product of human-like thinking.
This makes it hard for clinicians to challenge or validate AI decisions. Without clear, explainable pathways for how a diagnosis was reached, AI risks undermining trust, especially in complex or controversial cases.
Implications for Healthcare Organizations
So what does all this mean for healthcare institutions, payers, and public health leaders?
First, it’s clear that AI has transformative potential. But it’s equally clear that integrating AI into diagnostic processes carries real risks — financial, ethical, legal, and clinical.
Strategic and Operational Impacts
- Workforce Redefinition: AI doesn’t replace clinicians — it changes what they do. Future clinicians may need training not only in medicine but in data interpretation, AI oversight, and digital ethics.
- New Liability Frameworks: If an AI system contributes to a misdiagnosis, who is responsible — the vendor, the provider, or the institution? Legal clarity here is still evolving.
- Infrastructure Overhaul: AI integration requires more than a plug-and-play API. It needs secure data pipelines, real-time EHR integration, and continuous monitoring. Smaller clinics and underfunded hospitals may struggle to keep up.
- Cost-Benefit Reevaluation: Although AI can lower diagnostic testing costs, it may increase overall expenditures through licensing fees, implementation efforts, and ongoing maintenance.
- Governance and Ethics: Institutions will need formal AI governance teams to ensure systems are transparent, validated, and accountable — a new layer of oversight in already complex environments.
Zarego’s View: Augmentation, Not Autonomy
At Zarego, we’ve been closely following the evolution of AI in healthcare — both the hype and the hard truths. We believe the real opportunity lies not in replacing human expertise, but in augmenting it.
We’re optimistic about the future of diagnostic AI — but cautious about its deployment. When thinking about responsible adoption, we advocate for phased implementation, rigorous validation, and human-AI collaboration. The principles we use to guide our thinking and design approach include:
- Human-in-the-loop design: AI should support, not substitute, clinical reasoning. Systems must keep clinicians in control, with clear explainability and override functionality.
- Ethical engineering: Responsible AI requires attention to bias detection, data diversity, and risk assessment to ensure fair outcomes across patient populations.
- Transparency-first architecture: Diagnostic systems should be auditable and accountable — from logging AI recommendations to tracking their real-world impact.
- Practical integration: AI tools should be built to work within existing clinical workflows and environments — not just as proof-of-concept demos, but as part of sustainable, usable systems.
How We Support Healthcare Teams
Whether you’re evaluating a diagnostic AI tool, exploring automated triage, or building AI-enabled telehealth experiences, Zarego can help you assess what’s feasible, ethical, and sustainable.
Our team blends deep technical expertise with a grounded understanding of how healthcare actually works — not just in theory, but in practice. We help institutions:
- Prototype AI-enabled workflows with safety checks
- Build interoperable systems with major EHR platforms
- Train clinical teams in AI literacy and risk management
- Design governance policies and ethical oversight boards
Let’s Talk About the Future — Responsibly
AI is no longer a theoretical possibility in healthcare — it’s a present reality. But how we adopt it will determine whether it enhances care or undermines it.
For decision-makers, the challenge is to lead with clarity, ethics, and pragmatism. Don’t be dazzled by performance benchmarks alone. Ask harder questions: Who does this serve? What are the risks? How will we know it’s working?
At Zarego, we’re here to help healthcare organizations navigate these questions — and shape an AI future that’s innovative, safe, and human-centered.
Want to talk about how AI can fit into your clinical roadmap — not just your tech stack?
